The Time Is Past Due For Hospitals To Take Care Of Health Care Workers’ Mental Health Needs

Quel est votre défi ?
Since the pandemic began in early 2020, 20% of health care workers–doctors and nurses, admins and janitorial staff, case workers and mental health providers, and everything in between–have left their jobs. For hospital systems across the U.S., these numbers are alarming, causing staffing shortages and dangerous patient care environments.
According to Morning Consult, 19% of the healthcare workers (HCWs) who have stayed employed want to leave the healthcare industry altogether, and only 31% of the workers who have stayed employed had not considered leaving their current jobs.
A large impact on these feelings and the overall well-being of HCWs is burnout. For instance, according to a survey by Medscape and published in the report “Physician Burnout & Depression Report 2022: Stress, Anxiety, and Anger”, overall burnout is on the rise for physicians. For emergency room physicians specifically, the reported rise in burnout went from 43% to 60% over the course of a year.

Making up for lost time: provider shortages
Along with burnout, health systems are suffering after an entire generation of missed opportunities to expand the number of physicians practicing in the U.S. due to a lack of enrollments allowed in medical school programs.
One would think as the population in the U.S. steadily rose, you’d want enrollment for qualified med school applicants to rise as well. However, as reported by Dr. James Dalen, M.D, MPH in a commentary for the American Journal of Medicine, there was a “moratorium” placed on medical school enrollment from 1980-2005 due to “multiple predictions of an impending US physician surplus.”
This “moratorium” clearly had an adverse effect as we are now dealing with a growing shortage of physicians in the U.S. In fact, the Association of American Medical Colleges (AAMC) reported in 2020 that the deficit could be anywhere “between 54,100 and 139,000 physicians, including shortfalls in both primary and specialty care, by 2033,” which is extremely frightening to say the least.
Furthermore, the increased strain on hospitals as they experience their “great resignation” of HCWs means that those remaining already drained staff members, may have to cover off-hour shifts that they are not used to filling, further exacerbating their burnout.
A system on the brink
As a mental health professional myself, I can fully empathize with the struggles these HCWs are facing every day. There were times I was working with clients in individual or group settings where I experienced burnout simply due to the work itself, without the added pressure from outside factors like a global pandemic. The intense feelings of sadness, isolation, and hopelessness brought on by Covid-19 must be unbearable at times, leaving many providers to feel forgotten by the systems of care they have dedicated their lives to.
What you have here is a current blow to the system that is teetering on the brink of exploding into a full-blown disaster going forward for the industry. The impact of all of these factors must draw more attention from healthcare administrators, for the mental health and emotional wellbeing of their clinicians and staff.
A box may be checked in offering HCWs access to traditional mental health resources like therapy, but there are systematic obstacles to the usage of these services, including scheduling and overall stigmatization of needing care as a professional with mental health struggles.
Why healthcare systems need to provide HCWs different solutions
In 2020, The Washington Post reported that around 90% of physician state licensing boards ask about applicants’ mental health history during the application process. Furthermore, physicians may be asked to share documentation from their private mental health therapy sessions, and placed in a Physician Health Program (PHP) for more support or risk losing their medical license.
As reported in a 2018 review from the Journal of the American Academy of Psychiatry and the Law (JAAPL): “This questioning…is also inconsistent with the views of the American Psychiatric Association (APA), which says that having a psychiatric history is not an accurate predictor of mental fitness and, accordingly, status questions are inappropriate and irrelevant to the question of current impairment.”
Longstanding stigma poses an even greater threat to HCWs as the pandemic drastically impacts mental health. A poll from the American College of Emergency Physicians (ACEP) and Morning Consult gave some alarming data for Physicians working in the ER. 87% felt more stress since Covid-19 began, and 57% reported concern with job security if they sought mental health treatment.
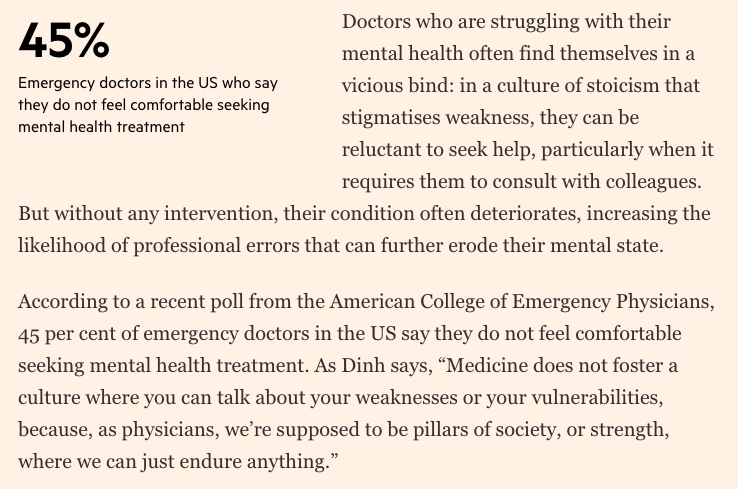
Given medical professionals’ well-known reluctance to obtain traditional mental health support (due to stigma, bias, and fear), it seems to me that hospital systems need to offer another kind of support to their HCWs–one that safeguards against judgement and mental health prejudice.
The best option would seemingly be one that is anonymous and available on demand and 24/7/365. One such option is Supportiv’s peer-to-peer support mental health service. Through Supportiv chats, a user (peer) is matched with other peers (HCWs in this case) going through a similar struggle to minimize emotional distress and deliver purpose to the user.
Professional real-time moderators guide the peer conversations from active listening and validation to coping, healing, and collaborative problem solving. Moderators drop customized resources (articles, videos, etc.) into the chat in real-time for either the whole group, or one peer specifically to best ensure that all needs are being met. As Supportiv users, you get the dual benefit of releasing those stressful and emotionally debilitating experiences, while listening to and helping other HCWs that are sharing their similar struggles in the chat.
How can healthcare systems adapt to meet HCW needs?
While hospitals may feel they are unequipped to roll out new protocols and initiatives during this time as no one will listen, they are mistaken. The harsh reality is many hospital systems may not make it through this time without looking at innovative, new ways to meet the needs of their healthcare staff.
When I was seeing clients, I felt great relief from consulting with my coworker peers on the emotional concerns that felt appropriate to discuss at work–like stress or fatigue. I saw the importance of the ability to have vulnerable discussions in the moment with others who had the same lived experience. But I never felt comfortable asking my work peers for situational support through more personal everyday life struggles. Talking about, say, the death of a family member, or even difficulties at work, felt off-limits. My employers never offered a venue to support those more vulnerable conversations.
What if there was a solution that could make that vulnerable connection feel free of stigma and risk of judgement? And, again, what if this solution could be available on-demand at any time of day, unlike therapy?
That’s where Supportiv comes in.
At Supportiv, we offer anonymous, peer-to-peer chats for health care workers to preserve their overall emotional well-being. This option allows HCWs the freedom to get immediate assistance when they need it, and the comfort of speaking with others that are going through those same concerns in real time.
Supportiv’s peer support network, tailored to healthcare providers and customizable by healthcare systems, provides simultaneous anonymity plus struggle-, person-, and occupation-specific peer matching. Supportiv users already include healthcare workers in 5 states, ensuring accurate occupational matching and a large pool of available peers who empathize with career-related emotional struggles. Improving HCW mental health improves not only overall health, but also the quality of care they are able to provide.
Without a psychological safety net for their staff, hospitals risk having their HCWs move out of their systems of care completely, and immediate peer support can greatly safeguard that from taking place.
Written by William Taylor, LPCC, NCC, VP of Strategic Partnerships at Supportiv.